The COVID-19 pandemic has prompted the rapid development and administration of various vaccines worldwide, with some reports linking these vaccines to immune thrombotic thrombocytopenic purpura (TTP).

This report presents two cases of TTP occurring after the administration of the inactivated vaccine CoronaVac from Sinovac Biotech, highlighting the potential association between this type of vaccine and TTP.
READ MORE: New study to examine very rare adverse events linked to COVID-19 vaccines
READ MORE: New study provides insight to why Covid vaccines hit some harder than others
The article also provides an analysis of TTP incidence in the Nanjing area of China, suggesting a possible correlation between COVID-19 vaccination and the occurrence of TTP.
Symptoms of TTP
The first case details a 23-year-old female who developed symptoms of TTP three days after receiving her second dose of CoronaVac. Initially presenting with dizziness and weakness, her condition progressed to include thrombocytopenia, anemia, elevated lactate dehydrogenase (LDH), and α-hydroxybutyrate dehydrogenase (α-HBDH) levels, with further deterioration indicated by decreased platelet count, hemoglobin levels, and the presence of schistocytes in peripheral blood smears.
Despite negative SARS-CoV-2 PCR test results, the patient was treated with dexamethasone, intravenous immunoglobulin, and platelet transfusion. Her condition improved following the introduction of glucocorticoids, plasma exchange, and rituximab, with a gradual return to normal values for ADAMTS13 antigen and inhibitory antibodies.
Fever and muscle soreness
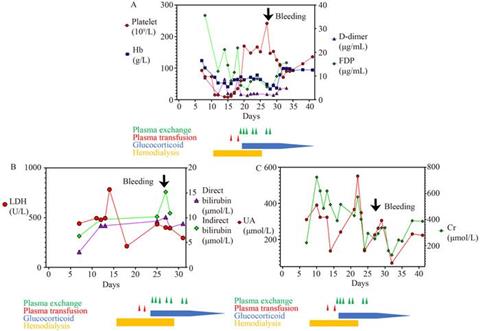
The second case involves a 45-year-old female who experienced fever and muscle soreness five days after her second dose of CoronaVac. She presented with high fever, hematological abnormalities, acute renal failure, and thrombocytopenia.
Despite negative SARS-CoV-2 PCR test results and initial suspicions of hemorrhagic fever with renal syndrome (HFRS) or severe fever with thrombocytopenia syndrome (SFTS), she was later diagnosed with TTP based on the presence of schistocytes in peripheral blood smears and significantly low ADAMTS13 levels. Treatment with plasma exchange and glucocorticoids led to her recovery, although she experienced a retroperitoneal hemorrhage that required surgical intervention.
Increase in incidence
The report also examines a series of TTP cases from 14 hospitals in the Nanjing area, showing an increase in TTP incidence from 2019 to 2022 that may be related to COVID-19 vaccination. The data suggests that while TTP is rare, with an average annual incidence of about one new case per million people, the incidence rates increased in years following the initiation of COVID-19 vaccination campaigns. It is hypothesized that the increase in TTP cases could be associated with the vaccines, although a direct causal link is not established.
Discussion within the report delves into the potential mechanisms by which COVID-19 vaccines could trigger TTP, focusing on the autoimmune response that may cross-react with ADAMTS13, leading to its deficiency and subsequent TTP development. The report also emphasizes the importance of accurate and timely diagnosis of TTP, as misdiagnosis can lead to inappropriate treatment, which may exacerbate the condition. Furthermore, it underscores the critical nature of plasma exchange and immunosuppression in the treatment of TTP, as evidenced by the successful management of the reported cases.
Insights into TTP
In conclusion, this report presents the first known cases of TTP associated with an inactivated COVID-19 vaccine and contributes to the growing body of knowledge on the potential adverse effects of COVID-19 vaccines. It also provides valuable insights into the diagnosis and treatment of TTP, highlighting the need for vigilance and appropriate clinical management in the context of COVID-19 vaccination programs.
The findings suggest a potential link between COVID-19 vaccination and TTP incidence, warranting further investigation to understand the mechanisms involved and to guide the development of strategies for the prevention and management of vaccine-related TTP.






No comments yet